Diabetes mellitus is a complex, progressive disease that affects every primary care provider’s practice. Major diabetes organizations recommend that treatment be ongoing and progressive in order to control the disease. The American Diabetes Association (ADA), the European Association for the Study of Diabetes (EASD), and the American Association of Clinical Endocrinologists recommend that patients be assessed every two to three months after diagnosis and that treatment should be intensified if the patient is not meeting treatment goals.1,2 Using this approach, all people with type 2 diabetes could be on insulin one year after diagnosis.1,2
While many clinicians have become comfortable with using once-daily basal insulin, such as glargine or detemir, what to do after basal insulin is much more complex. This review explains three strategies to consider when basal insulin alone isn’t enough.
3 MAIN STRATEGIES FOR INTENSIFYING TREATMENT
Basal insulin is indicated for patients who have glucose toxicity and persistently elevated A1C despite using two or more oral agents or for those who have not achieved glucose goals one year into treatment.3,4 ADA/EASD recommends initiating a weight-based approach for basal insulin therapy based on initial A1C levels > 7% or > 8%.4 Instructing and encouraging patients to titrate their own insulin dose based on fasting glucose readings provides greater and faster glucose control.1,2
Despite these attempts, some patients will not reach their glucose goals with basal insulin. When intensifying treatment beyond basal insulin therapy, patient preference, cost-effectiveness, safety, tolerability, glycemic efficacy, risk for hypoglycemia, effects on cardiovascular risk factors, and other nonglycemic effects should be considered in the shared decision-making process. There are three main strategies for intensifying treatment:
Basal plus incretin therapy. Add a newer injectable agent, such as a glucagon-like peptide 1 receptor agonist (GLP-1RA).
Basal plus one strategy. Add prandial insulin prior to the largest meal of the day.
Basal-bolus combination. Add insulin prior to all meals.
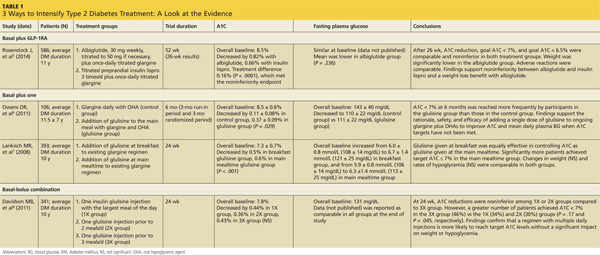
Table 1 provides details of several studies that have documented the efficacy of these three strategies.5-8
Monitoring blood glucose to guide the way
Blood glucose monitoring using a 7-point glucose monitoring technique or staggered glucose checks should guide insulin intensification. A 7-point glucose profile includes pre-meal and post-meal readings for three meals a day and an additional bedtime reading.9 This is typically performed for three to seven days prior to an appointment and provides an estimate of a typical full day’s glucose pattern.
Staggered monitoring includes a pair of glucose checks taken immediately before and typically 90 minutes after a meal. This is assigned to a different meal each day in order to obtain the same information as is achieved with 7-point monitoring, but with fewer checks on any given day. It may take up to two to three weeks to gather the necessary information using the staggered monitoring technique.
In order to optimize insulin strategies for tighter glycemic control, it is important to review blood glucose logs at each office visit with either of the above techniques.
BASAL PLUS INCRETIN THERAPY
GLP-1RAs are subcutaneously administered injectable incretin agents. They mimic the action of endogenous GLP-1 hormones, which are normally secreted in response to meals by the cells of the small intestine.10 GLP-1 stimulates glucose-dependent insulin secretion, suppresses postprandial glucagon release from pancreatic alpha cells, signals satiety, and slows gastric emptying.10 In other words, GLP-1 appears to be a physiologic regulator of appetite and food intake. GLP-1 is rapidly metabolized and inactivated by dipeptidyl peptidase-4 (DPP-4) enzymes.10 The amplification of insulin secretion elicited by hormones secreted from the gastrointestinal (GI) tract is called the “incretin effect.”10 Obesity, insulin resistance, and type 2 diabetes greatly reduce the incretin effect.10
GLP-1RAs mimic the incretin effect and are not degraded by endogenous DPP-4 enzymes.10 They provide a pharmacologic level of GLP-1 activity, including beneficial glucose effects (via insulin secretion and glucagon suppression), but they also increase GI adverse effects, such as nausea and vomiting.11-15 Further, they can suppress appetite and contribute to weight loss.11-15
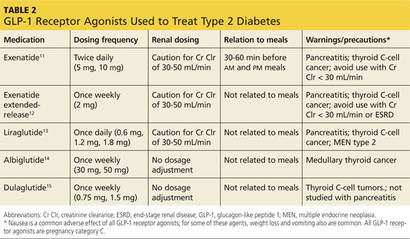
GLP-1RAs can be considered as add-on therapy for patients whose A1C exceeds 7% and whose fasting blood glucose ranges from 80 to 130 mg/dL or those with a basal insulin dose > 0.5 U/kg/d. The five currently available GLP-1RAs (exenatide, exenatide extended-release, liraglutide, albiglutide, and dulaglutide) are compared in Table 2.11-15
Dosing varies with each agent and includes twice daily before meals for exenatide, once daily (independent of meals) for liraglutide, and once weekly for exenatide extended-release, albiglutide, and dulaglutide. These agents should not be used for patients with a history of pancreatitis or a personal or family history of medullary thyroid cancer or multiple endocrine neoplasia type 2. Because exenatide is cleared through the kidneys, its use is contraindicated in patients with a creatinine clearance < 30 mL/min or end-stage renal disease. Caution is advised for its use in patients with a creatinine clearance of 30 to 50 mL/min.11
Continue for basal plus one strategy >>